

Mucho la bandha, which muscles are involved and where they are located. In translating the original Sanskrit texts many commentators, being unfamiliar with yogic practices or not fully conversant with the basic anatomical aspects of the pelvic floor, have unknowingly led people to believe that there are two ways to practise moola bandha when, in fact, there is only one.
Many translations of hatha yoga texts describe moola bandha as pressing the heel against the perineum and contracting the anus. It should be carefully noted, however, that this practice is ashwini mudra.
The ancient tantric texts (the scriptural foundation of kundalini yoga and kriya yoga) reveal that moola bandha is performed by relaxing the anus (sphincter muscles) and contracting only the perineal body.
As the scriptures did not clearly differentiate anatomically between the sexes, some confusion has arisen over how moola bandha should be practised by males and females, owing to anatomical differences. Scriptural descriptions all relate to the male body. In the male the heel is placed against the perineum behind the scrotum and in front of the anus. In the female it is also placed in the perineum, pressed against the outer vagina. The perineum is a group of muscles which extends the entire length of the pelvic floor, related to both the urogenital and anal areas.
It is not a single muscle. Moola bandha is not contraction of the whole perineum as this contraction will bring about moola bandha as well as vajroli mudra and ashwini mudra. The actual point of physical contraction varies according to sex. In the male it is the perineal body while in the female it is the area around the cervix. When the average person contracts the anal sphincters the perineum is also involuntarily contracted.
Because contraction of the perineum is difficult for the beginner, the first exponents of hatha yoga, realizing the interconnection between the anal sphincters and the perineum, recommended contraction of the anal muscles (ashwini mudra) thereby leading to an involuntary contraction of the perineum. Personal exper ience, however, will verify that the direct (conscious) contraction of the perineum has a distinct effect on the physical and mental bodies, different from that of the indirect method of contracting the anus. Contraction of the anus is a necessary preparation for the more subtle and difficult practice of moola bandha.
Perineum and perineal body
It is indeed important to have a clear picture in your mind of the basic muscle structure of the lower pelvis or perineum, not only in order to practise moola bandha correctly, but also in order to understand the anatomical interrelationships between moola bandha with ashwini and vajroli mudras, two techniques also performed in the area of the lower pelvis.
The perineum overlies the outlet of the pelvis. Its internal boundaries are in front of the pubic arch (the bone slightly above the genitalia) and behind the tip of the coccyx (tail bone). Its external boundaries are the scrotum/clitoris and the buttocks.
The muscles of the perineum are divided into two groups:
- Those of the anal region – found at the end of the gastrointestinal tract.
- 2. Those of the urogenital region – around the urinary and sexual organs.
The muscles of the anal region, the larger of the two groups, and the muscles of the urogenital group are connected by fibrous tissue and are interrelated to the extent that movement of one group usually elicits a response from the other. Thus, controlled movement of one area alone requires considerable skill. The muscles of the perineum are normally utilized only on the occasions of urination, defecation and ejaculation/orgasm.
We have not been taught to consciously isolate pelvic muscle groups with the same exactness as we have the muscles of the arms and legs, which we use continually in specialized, conscious daily activity. The reason why most people find precise nervous control over the perineum more difficult than that of the arms and legs may be due to the fact that the areas in the brain associated with the motor activities of the perineum are small when compared with the larger, more developed areas regulating the arms, hands and face, allowing finer movements and better control. By regular practise of moola bandha the area in the brain associated with the perineum will develop so that one may gain complete control over such processes as urination, defecation and sexual intercourse. The pelvic muscles are mainly required for all subconscious and unconscious autonomic activity. This lack of conscious nervous control makes it difficult for a person to both urinate and defecate at the same time.
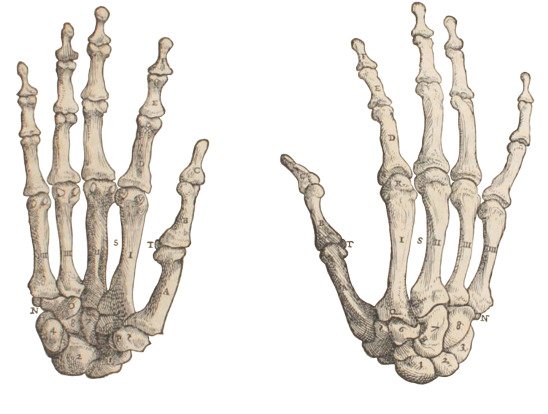
The implication of this for the yoga beginner is that the contraction of one set of perineal muscles involves the involuntary contraction of the other. We can better understand this when we remember that the third and fourth toes are joined by fibrous tissue and it is extremely difficult without practise to move one without moving the other. Because of the interconnection of muscles and other fibrous tissue and lack of precise control over the nerves in the perineum, it is difficult to perform vajroli or ashwini mudras without performing moola bandha at the same time. This applies equally to men and women.
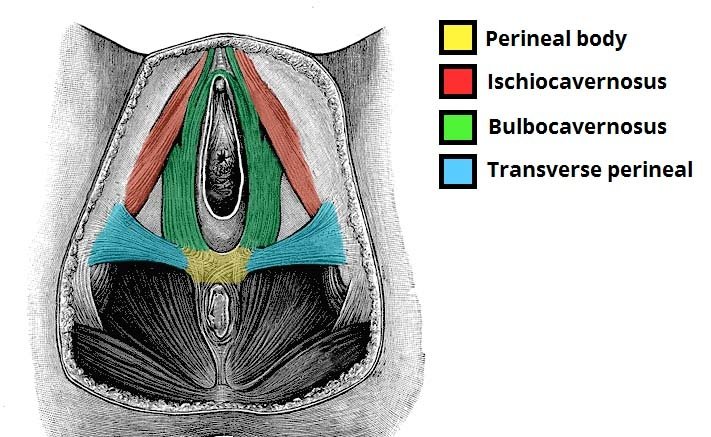
It is necessary to fully appreciate the fact that the perineum is not one muscle but a group of muscles which are common to both sexes. Likewise, there exists a clear distinction between the perineum and the perineal body or central tendon of the perineum. In the male and female the perineal body is a small fibromuscular node about one to one and a half inches in front of the anus and approximately two inches inside the body.
Towards this point the pelvic muscles converge and are attached: the superficial and deep transverse perineal muscles, bulbospongiosus, the external anal sphincter and the levator ani. The rectum also sends some of its muscle fibres to this central and vitally important structure, which divides the urogenital area from the anal region.
It is a compact complete node, and its importance to the pelvic floor in the female is such that if damaged or torn, as in pregnancy for example, it may cause the uterus, ovaries and/or rectum to prolapse (slip out of place). Therefore the perineal body, especially in the female body, plays a very important role and is the pivot around which everything is joined or supported.
In the male, the perineal body is the trigger point for mooladhara chakra. In the female, however, the back of the neck of the womb or cervix, rather than the perineal body, is the trigger for mooladhara chakra.
Anatomical aspects refined
Having discussed the perineum and the perineal body, we can now explore in finer anatomical detail the distinguishing areas of the three different yoga practices that are performed in the region of the pelvic floor: vajroli mudra, ashwini mudra and moola bandha.
The muscles contracted in these three practices are: • Ashwini mudra: The anal area including the following muscles: sphincter ani externus and levator ani which consists of the pubococcygeus, iliococcygeus and puborectalis, i.e. the anal muscles are contracted.
Moola bandha: The area between the anus and scrotum/ clitoris, the perineal body/cervix is contracted. Vajroli mudra: The urogenital muscles including the transversi perinei superficialis, ischiocavernosus, bulbo spongiosus, transversus perinei profundus and the sphincter urethrae, are contracted. In the male the penis is slightly contracted inwards; in the female, the clitoris, lower vaginal muscles and the urethra are contracted.
The actual location of these muscles can best be described by personal experience. Whenever you have to consciously withhold the onset of urination or defecation you become acutely aware of the muscles necessary for both vajroli mudra (preventing urination) and ashwini mudra (preventing defecation). It is difficult to release both these muscle groups at the same time (though structurally it is possible).
Once, however, either of these muscle groups is relaxed (urogenital is usually the first), the excretory process may take place. When excretion has concluded, both vajroli and/or ashwini again spontaneously occur for a short time.
Moola bandha: men and women
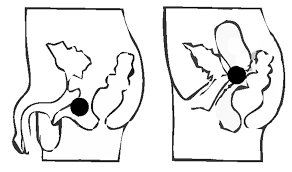
Embryologically the penis and vagina are formed from the same structure while still in the foetus. When hormonal activity begins, the basic genital structure forms according to the sex of the foetus which has already been determined at conception.
Thus, despite the different formation of sexual organs, the basic muscle structure of the lower pelvic region is the same for male and female and the vagina occupies approximately the same area as the root of the penis. The neurological and hormonal connections with this area are likewise the same for both sexes.
Conclusion

In the beginning the student will find difficulty in asserting conscious control over the perineal area as the brain is not tuned to such fine muscular manipulation in this area.
The practice of moola bandha reactivates the areas in the brain controlling this lower region of the body, bringing the neuronal circuits responsible for its control into the sphere of consciousness.
This growth process takes time and in the meantime, while practising moola bandha, it is important not to become frustrated if you cannot contract the perineal body or the cervix without contracting the anus or genital organs also. In the initial stages of practice this is to be expected. Be assured that control will definitely come with time, practice and perseverance.
Can you be more specific about the content of your article? After reading it, I still have some doubts. Hope you can help me.
I am a website designer. Recently, I am designing a website template about gate.io. The boss’s requirements are very strange, which makes me very difficult. I have consulted many websites, and later I discovered your blog, which is the style I hope to need. thank you very much. Would you allow me to use your blog style as a reference? thank you!